Female Circumcision is removal of the hood of the clitoris to expose the clitoral glans; an operation exactly equivalent to male circumcision. However because the term has also come to be applied (incorrectly) to forms of female genital mutilation (FGM) it has acquired a pejorative association and alternative terms such as 'hoodectomy' are more acceptable.
Labiaplasty is the reduction of the labia minora (inner lips). In some women they project beyond the labia majora (outer lips) to an extent which may be seen as unsightly, and can also be uncomfortable. The operation is becoming increasingly popular, especially in the US. In the Australian state of Queensland, depiction of protruding inner lips is actually illegal (!) so Penthouse models have to face having their pictures retouched if they have this "problem". While this surgery is usually cosmetic, and is not actually circumcision, we mention it here since it is usually combined with hoodectomy.
Female Genital Mutilation, FGM applies, strictly, to two different procedures, clitoridectomy and infibulation. These have attracted huge media attention although they are actually only practised in a few countries. The media attention has arisen, in part, because of a huge exodus of refugees from war-torn Sudan.
Clitoridectomy is the excision of the external portion of the clitoris. This seriously reduces a woman's capacity for sexual response. It is practised in Egypt, but the extent of the practice elsewhere is not clear.
Infibulation involves clitoridectomy followed by labioplasty and then closure of the labia majora so that sexual penetration is impossible. An opening is left for passage of urine and menses but this is often inadequate so that manual dilation is required for urination and menses are retained. This barbaric practice has attracted widespread media attention to the extent that it has become seen as 'female circumcision'. In actual fact it is only practised in parts of Somalia and Sudan .
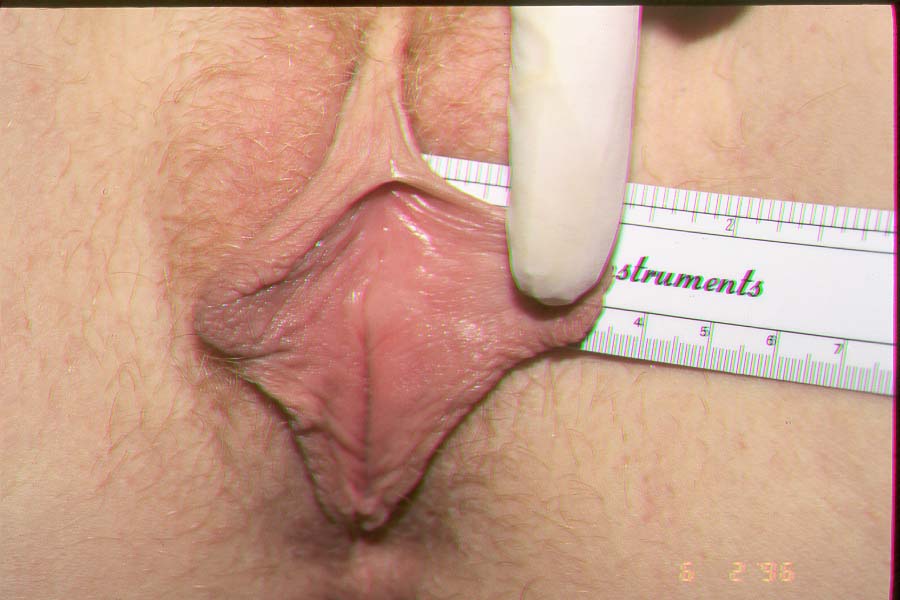
Hoodectomy -unhooding of the clitoris - true female circumcision
Medical and aesthetic hoodectomy and labiaplasty
Serious attention began to be paid to the clitoris and its foreskin in the 1950s. Initially, phimosis and attending infection were the main target. In 1958
C.F. McDonald wrote "When we were interns, 33 years ago, the staffroom conversation one day came around to the clitoris of the female infant. As I remember, the sum total of knowledge of the subject among those present was zero." He carried out a procedure, with anaesthetic, which essentially forcibly broke apart the adhering part of the hood, without removing anything. It soon became apparent that as well as dealing with infection and accumulated smegma, he was also vastly improving the sex lives of his patients. This latter consideration was behind the promotion of hoodectomy by American doctor
W.G. Rathmann in 1959. He felt that excessive or phimotic clitoral foreskin was a major cause of anorgasmia and consequent marital difficulties. His enthusiasm seems a bit comical today - hoodectomy would, in his view, avoid 70% of American divorces! But subsequent reseach has borne out the fundamental premise. 41 years later, in 2000,
Scientific American reported on a study of 200 women attending a sexual dysfunction clinic which found that a quarter suffered from clitoral phimosis. Hoodectomy is now a well established practice, and images and a list of doctors performing 'hoodectomy' in the USA can be found at
clitoralunhooding.com. A web search will find specialist clinics in other countries.
Women whose
labia minora are long enough to protrude beyond the outer lips may seek to have them reduced for aesthic or comfort reasons - often both. The procedure first became known in the 1980s with a medical paper by
Hodgkinson and colleagues but it really hit the public eye in 1998 following publication of an article in the North American edition of
Cosmopolitan magazine, quoted in the
Toronto Globe and Mail. While labiaplasty is not circumcision (the labia are developmentally equivalent to the male scrotum), it is usually combined with hoodectomy and so rates a mention here. A web search will reveal local clinics which perform the procedure.
A previous version of this page suggested that these procedures might be illegal even on adults in Britain following a law of 2003. However dozens of UK clinics still offer hoodectomy and labiaplasty so this seems over alarmist.
Islamic female circumcision
The world's most populous Islamic country is Indonesia, with a population of 250 million, 210 million of whom are Muslim, though there is a substantial Christian minority, and the island of Bali is predominantly Hindu. The government is somewhat anti religion, and female circumcision is officially banned. However the Islamic Council states that female circumcision is mandatory and in practice the government does nothing to enforce the ban. Circumcision of girls is carried out on babies, whereas boys are circumcised between ages 5 and 10.
Although it is written from a strongly anti-circumcision viewpoint, a
recent article gives an accurate description of the Indonesian practice. While the extent of cutting varies, "We don't touch the clitoris" is the response of every practioner. The practice in medical contexts varies from a removal of part of the hood to a purely symbolic prick with a needle, though some traditional midwives remove all of the foreskin "like circumcising a boy".
Neighbouring Malaysia is much smaller (30 million), but is formally a Muslim country and female circumcision is both mandated by the religious authorities and permitted by the state. Current practice has been described by
Sya Taha. Essentially, part of the clitoral hood is removed so that the tip of the clitoris is exposed. It is hard to see this as anything but life-enhancing. Nothing is done to the inner labia in either Indonesia or Malaysia, but then south-east asian women generally have only minuscule
labia minora.
What of other Muslim countries? Pakistan, population 200 million, is the second largest Muslim country, and there female genital modification is only practiced by one tiny sect, the Bohra Muslims. In Bangladesh, population 160 million, it seems not to be practised at all. In Iran, population 77 million, which follows the Shiite Muslim tradition, it is practised only by the Sunni minority, and then not in any harmful form.
These sober figures make nonsense of the pages and pages of hysterical writings claiming, in a mixture of anti-circumcision fervour and islamophobia, that Muslim girls are mutilated. At least half, probably more, either have nothing at all done to them or else receive a purely symbolic needle prick. Those that are operated on have their clitoral hood reduced, an operation that women in the West are queueing up to pay big dollars for. The latter group are the lucky ones, since their sex life will be greatly enhanced. (Just as it will be for their circumcised brothers).
This all presents a problem for the Western doctor who cares more for his/her patients that for rhetoric, and this was spelled out very clearly in a
letter to the British newspaper the Daily Telegraph. The London gynecologist was asked by a Nigerian woman to 'circumcise' her daughter. Because 'female circumcision' is so widely used to refer to one of the several versions of FGM - and because all such surgeries are illegal in Great Britain - the doctor refused the woman's request. The mother was 'puzzled and upset' by his 'stern and abrupt' refusal to perform the surgery.
It was only when he conducted a gynaecological examination on the mother that he realized how circumcision carried out at the age of thirteen had made this 'smiling, nubile, satisfied wife' a 'very happy woman,' and why she wanted it for her daughter. The operation had been carried out under a local anaesthetic, and all that had been removed were the labia minora and the hood of the clitoris. The clitoris itself had not been excised. The effect, he reported, was that 'any possible obstruction to the woman's (and her husband's) pleasure had been removed.' The gynaecologist commented 'Perhaps there's more than one way of doing this controversial operation.'
The following image was placed on Facebook by a Muslim women's association, but was forcibly removed. We present it here as a reasonable statement of the Muslim female viewpoint.
References
Raquiya Haji Dualeh Abdalla, Circumcision and Infibulation of Women in Somalia. in Sisters in Affliction, Zed Press, London 1982. pp 7-29
Asma El Dareer, Woman why do you weep? Zed Press, London, 1982, 106pp
McDonald, C. F. 1958 Circumcision of the Female. General Practitioner 18.3 98-99
Rathmann, W. G. 1959 Female Circumcision, Indications and a New Technique. General Practitioner 20.3 115-120. full text here
Carol Ezzell, Anatomy and Sexual Dysfunction, Scientific American, October 31, 2000. full text here
Hodgkinson, D.J. & Hair, G, 1984. Aesthetic vaginal labioplasty. Plastic and Reconstructive Surgery 74, 414-416
Toronto Globe and Mail Tuesday, 10 November 1998 "New hot cosmetic surgery for women" by Krista Foss, Health Reporter full text here
Marie Dhumieres, Female genital mutilation persists in Indonesia GlobalPost 10:27 a.m. EDT April 16, 2015 reprinted in USA Today
Sya Taha, A Tiny Cut: Female Circumcision in South East Asia
The Islamic Monthly, March 12, 2013 original article
Dr. William A. R. Thompson, Female Circumcision: Airing the Doctor's Dilemma. The Daily Telegraph, May 4, 1983, 15.
Copyright © 1992 - 2017, All Rights Reserved CIRCLIST.